Trinômes to Binômes: Optimizing Community Health Resources to Achieve Universal ITN Coverage in the DRC

A cohort of two health workers, or binôme, sensitizes a family in the Lualaba Province of the DRC on the benefits of sleeping under an insecticide-treated net (ITN) every night. One member of the binôme hands them an ITN while the other records the visit, noting that the family received one ITN for every two people as established by international standards. Credit: Arlette Bashizi.
The DRC National Malaria Control Program successfully implemented a new structure for community teams distributing insecticide-treated nets that more efficiently uses its community health workforce and enhances malaria prevention efforts.
Despite having limited resources, the Democratic Republic of Congo (DRC) continues its fight against malaria through the widespread distribution of insecticide-treated bed nets (ITNs). However, finding efficiencies and reducing the cost of each campaign is paramount. Thanks to the collaborative efforts of the U.S. President’s Malaria Initiative (PMI), the Chemonics-led USAID End Malaria Project, and the DRC National Malaria Control Program (NMCP), a significant milestone has been reached: the transition from a team of three community health workers (CHWs), or a trinôme, to a team of two, a binôme, for mass ITN distribution campaigns. This strategic shift signals a groundbreaking achievement, yielding 30% cost savings on both human resources and training costs for each campaign.
In February 2024, the NMCP and its stakeholders modified the national ITN distribution campaign manual. This shift to the binôme approach is a strategic move for the DRC, which has the second highest malaria burden globally, accounting for 12.3% of global cases and 11.9% deaths reported in 2022. Though effective, the use of trinômes, combined with other country context factors, made the campaign operational distribution costs in the DRC higher than in other countries such as Uganda. Resource optimization is imperative, especially when national organizations are working to ensure universal ITN coverage by 2030. Other NMCP partners, such as the Against Malaria Foundation committed millions of ITNs in the coming years and the binôme move will reduce the concerns on distribution resources currently being mobilized.
The path to binôme
Evidence-supported advocacy: Previously, the national policy required trinômes to distribute ITNs. In 2023, faced with a shortage of funds to support a campaign in Lualaba province, the End Malaria project, with support from USAID and PMI, advocated to the NMCP to explore ways to reduce operational costs. The NMCP granted the project permission to pilot the binômes model, provided it would deliver evidence on its effectiveness. In August 2023, the project piloted the binôme model in Lualaba and reached 97% of targeted households. In total, over 2.1 million ITNs were distributed, benefitting almost 4 million individuals—at an average of 1.8 persons per ITN—and exceeding the World Health Organization (WHO) recommendation for achieving universal ITN coverage. These results are not only comparable to previous campaign achievements utilizing the trinôme model, but also yield substantial cost savings while freeing up NMCP resources.
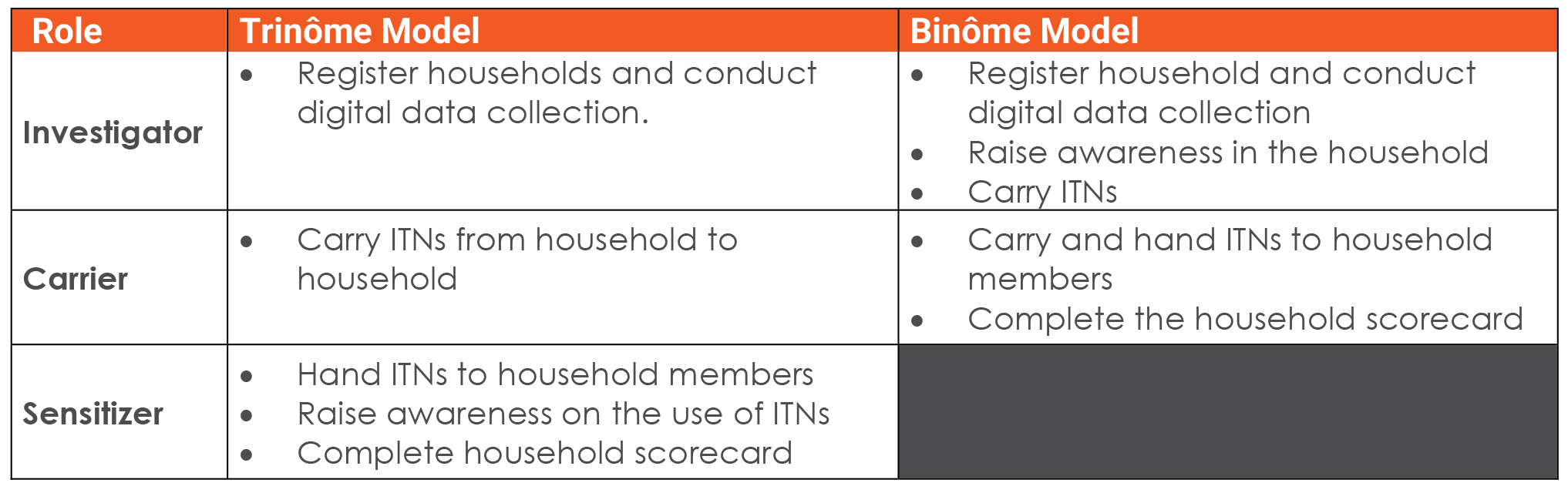
Role Revision: The change from trinômes to binômes required readjusting the community worker’s roles, and the End Malaria Project, in collaboration with PMI and the NMCP, modified the roles as follows:
The End Malaria Project also revised training materials and used them during cascade training activities in preparation for ITN distribution using the binôme model.
Pilot and scale-up: The project selected two of the 14 health zones, one rural and one urban, in the province to monitor potential bottlenecks and challenges. Throughout this initial phase, the project noted:
- Role clarity: 75% of CHWs completely understood their roles while 25% lacked clarity and encroached into their partner’s responsibilities.
- Recording accuracy: 88% of CHWs recorded data correctly.
- Time spent per household: 100% of binômes spent 12-15 minutes in the household, compared to the NMCP standard of 10-15 minutes for trinômes.
- Daily output: Each binôme completed between 25-30 households daily in rural areas against an NMCP target of 30 per trinôme team. In urban areas, the achievements were between 40-50 against a target of 50. However, the mass campaign was still completed within seven days as planned, except for a few health zones that routinely experience logistical issues.
The project reviewed successes and challenges and scaled up implementation to the remaining health zones in the province.
Binôme model direct savings
The table below shows the direct savings, primarily reflected in training costs, that resulted from the change to binômes during the Lualaba campaign.
 Direct savings translated to almost $222,000, a 33% decrease in operational costs. In addition to the costs, the use of binômes freed up more than 2,700 community workers, who could now focus on other critical activities in primary health care, such as vaccinations.
Direct savings translated to almost $222,000, a 33% decrease in operational costs. In addition to the costs, the use of binômes freed up more than 2,700 community workers, who could now focus on other critical activities in primary health care, such as vaccinations.
Lessons learned
The transition from trinômes to binômes was not without its challenges, including initial skepticism and resistance to change. However, the project overcame these obstacles through transparency, engagement, and adaptation. Key lessons learned included:
- Evidence-based advocacy, stakeholder engagement, and flexible programmatic approaches are important.
- Close monitoring and collaboration with national and local government is essential in generating evidence critical for timely change in national policy and guidelines.
- Although binômes could complete all campaign activities within the expected 7-day period, they experienced challenges meeting daily targets, requiring a reduction in daily targets from 30 to 25 households in rural areas and from 50 to 40 in urban areas.
The transition from trinômes to binômes represents a significant advancement in optimizing community health resources in the DRC while sustaining progress toward universal ITN coverage.